The veracity of non-peer-reviewed articles
from the Philippines and (supposedly) Indonesia and India regarding vitamin D and COVID-19
severity and deaths
Introduction
Please see the
#updates section at the end for pointers to the latest updates to this page.
An article published by Mark Alipio in the
Philippines
on 2020-04-08 has gained prominence in the debate about vitamin D and
COVID-19. It has been widely quoted and cited, including by me,
as if it was a genuine report of vitamin D levels and COVID-19 symptom
severity. In late June 2020, I formed the hypothesis that this article does not represent real research.
This was prompted by questions which arose about the veracity of a
second article, attributed to Prabowo
Raharusuna, Sadiah Priambada, Cahni Budiarti, Erdie Agung and Cipta Budi
(although the first author is also known as Prabowo Raharusun) of
Indonesia.
This lead me to similar questions about a third article by some authors ("Glicio" et al) in
India.
All three articles concerned the relationship between vitamin D levels
in the blood and the severity of COVID-19 symptoms. This is a
matter of great interest and importance. Although, in July 2020,
more research is now appearing concerning this question, there was
great lack of such research before this, which lead to the Filipino and
Indonesian articles being widely discussed and cited.
These three articles were published on the widely used and respected
SSRN preprint system, which is owned by Elsevier. The
Indonesian article was withdrawn in mid June and the Indian one ("Glicio") in
early July 2020.
In researching these articles I discovered 20 more by Mark Alipio, most
of which were about subjects unrelated to COVID-19 and vitamin D.
I have mentioned these below, because I believe that the article of his
which gained such prominence, number 16 of the series published in
March and April 2020, should be considered in the context of the others.
Despite extensive efforts, I was unable to find any evidence which
contradicted my hypothesis that all these articles (21 attributed to
Mark Alipio, one to "Raharusun" et al. and one to "Glicio" et al.) were
fabricated -
that the research they purport to report never took place. I
found numerous reasons to believe they were indeed all fake academic
research articles.
If anyone has arguments for the
veracity of these articles, on a public web page, forum or academic
article I will be happy to link to these. I
have spent a lot of time on these articles and am not interested in
engaging with further debate about their veracity or regarding their
authors.
On 2020-07-01 I created this website to host the page you are reading
now. This page was originally focused on both the
textual/diagrammatic content of the articles and on questions of who
wrote them, since I was not convinced that they were all written by the
person to whom their authorship is attributed.
This second set of concerns, about authorship, grew in complexity.
Since I believe the veracity of the articles can be shown to be less
than the standard expected, just based on the textual/diagrammatic
content, on 2020-07-12 I completely revised this page to focus jut on
this. However, I do mention the other 20 Mark Alipio
articles, one of the organisations he is affiliated with, and the
Indonesian hospital mentioned as the contact address for the first
author of the Indonesian article. I believe these are relevant
when assessing the veracity of the articles, since they tell me
something about the contexts in which the articles were
written.
For instance, if I had discovered that all the other 20 articles by
Mark Alipio were of excellent quality, then it would be harder to argue
that number 16's deficiencies were the result of the article being
fake. Also, if I had discovered that the hospital was a large,
well-resourced, teaching hospital with multiple MDs and other
researchers with a solid academic publishing history, then it would be
more difficult to argue that the deficiencies I found in the Indonesian
article were the result of it being fictional.
The question of authorship is important when evaluating the veracity of
academic research articles. Please see my thoughts on this at the
home page:
../#authorship .
Please see the home page
../#about for notes on how I am not an authority, have no formal qualifications etc.
Below (except for updates prompted by an auricle by three Indonesian
MDs and a subsequent document published on an Indonesian government
website) I proceed as if there are no questions about the identity of
the
ostensible authors or whether they wrote the articles. If these
questions interest you - and they may if you find the text and diagrams
of the articles meet your standards of academic rigour - then you will
need to research this yourself.
The veracity of academic articles in general, and these ones in
particular, is of interest to many people and so some of these articles
have been mentioned on other sites. I have not put much effort
into finding such sites, but here are two:
This mentions some newspaper articles
which quoted the Indonesian article it and how it was one of the most downloaded articles on
the SSRN print server.
Please link to this page and quote selectively from it rather than copy the
whole of its contents. I may update it and don't want old copies floating around on the Web.
To the ResearchVeracity.com home page:
../
This page established 2020-07-01. Simplified and revised 2020-07-12.
Last
update
2020-08-20.
Update history:
#updates
Robin Whittle Email:
rw@firstpr.com.au
. Daylesford, Victoria, Australia
The three articles from the Philippines, Indonesia and India
Here are the articles in date order:
1
Vitamin
D Supplementation Could Possibly Improve Clinical Outcomes of
Patients Infected with Coronavirus-2019 (COVID-2019)
Mark Alipio
2020-04-08 (Not peer-reviewed.)
Davao Doctors College; University of Southeastern
Philippines
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3571484 (Withdrawn around 2020-08-19.)
|
This is the 16th article in a set of 21 articles
#MA-list which were published on preprint servers over a period of 5 weeks in
late
March to late April 2020 with authorship attributed solely to Mark Alipio.
See:
#MA-critiques and
#MA-16-critique .
2
Important update 2020-07-27:
See the following article in which three Indonesian MDs find no trace
of the purported authors of the above article. This includes searching
the Indonesian Medical Council database and contacting the hospital
mentioned in the article:
COVID-19 and Misinformation: How an Infodemic Fueled the prominence of Vitamin D
Joshua Henrina, Michael Anthonius Lim and Raymond Pranata
British Journal of Nutrition 2020-07-27
https://doi.org/10.1017/S0007114520002950
|
See
#R-article and
#R-critique .
I am not aware of any other articles by any of Prabowo Raharusun,
Sadiah Priambada, Cahni Budiarti, Erdie Agung, Cipta Budi, or by any of
the authors of the next mentioned article from India
Important update 2020-08-03:
See the end of
#R-critique for three additional critiques of the "Raharusun" article from Dr Raymond Pranata.
Important update 2020-08-13:
See
#indon-govt
for a link to a document at an Indonesian Government website which
attests to the veracity of the
COVID-19 and Misinformation article and
establishes beyond doubt that there never was a doctor by the name of
"Prabowo Raharusun" associated with the hospital mentioned in the article, that the purported research is unknown to the
hospital and that the hospital does not and never did have a website.
This means that the website I and others assumed was the hospital
website was (since it no longer exists) fake.
3
Vitamin
D Level of Mild and Severe Elderly Cases of COVID-19: A Preliminary
Report
El James Glicio, MD; Siddharth Neelam, MD; Rajeev Rashi,
MD; Deepak Ramya, MD
No date on the PDF, but 2020-05-05 on the SSRN page. (Not peer-reviewed.)
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3593258 (Withdrawn in early July.)
|
Context
I had never encountered academic articles which were largely
or wholly fictional. Now I believe I have, I will be much more
cautious in the future.
The framework in which I am suspicious of some academic articles is
partly based on my understanding of the problems of predatory
journals. Here are some pages to get started on this important
field, which is a real threat to science and the pursuit of knowledge:
#MA13-similar
Update 2020-08-10:
Until 20220-08-10, the notes below
about none of these article being in journals was true. However,
today I found a Mark Alipio article which appears in a journal:
International Journal of Engineering Technology Research & Management.
The bold red Times typography is as the journal's name appears in the
PDF, which has a date of 2019-11-27, and is very similar to article 13
below.
To determine whether this was a predatory journal I tried to follow the first four investigatory steps suggested here:
https://mdanderson.libanswers.com/faq/206446
1 - The journal's name (including
searching for the first 6 words, to avoid possible glitches with
'&' and "and") does not appear in any search results from the
Directory of Open Access Journals:
https://doaj.org/search? Since the journal
presents itself as open-access journal, with publication fee, this shows that it is a predatory journal.
2 - Nor does it appear in the NLM Catalog
https://www.ncbi.nlm.nih.gov/nlmcatalog/ - again indicating it is predatory.
3 - Access to Cabell's blacklist is subscription-only so I did not consult it.
4 - Likewise the Journal Citation Reports database.
The journal's publication fee for authors outside India is 600 rupees,
which is about USD$8 (eight dollars). The title of this
article is
Locus of Control, Motivation and Academic Success of First Year Radiologic Technology Students . I found it at
academia.edu and
researchgate and
http://www.ijetrm.com/issue/?volume=November~2019 .
However the articles I discuss below, which I believe to be fake, are not directly related to
predatory publishing. They exist largely
or entirely outside journals - even
predatory journals. They are published primarily
or solely on preprint
servers, academia.edu (a commercial company which I think should not
have a .edu top level domain), researchgate.com and the like.
These articles may be related to the essay writing industry - since it
is possible to order a research paper, masters level, of specified
number of pages and subject matter, from companies which provide essay
writing services. In this way, a person who has never written an
academic article could post articles they purchase in this way, with
their name as author in the text of the document - and so build
an academic reputation of sorts.
For instance,
https://extraessay.com
offers an $11 a page, "plagiarism-free", essay writing
service. Masters level research papers cost $14 a page with a 14
day lead time. Delivery times as short as 3 hours are offered: USD$49 a page for a masters
research paper.
In fact, if anyone looks closely enough at such articles, the ostensible author's reputation will be less
than zero. However, too many people (in the past, myself
included)
don't look closely
enough at the article, cite it, and so add to the author's citation
count in Google Scholar and in other systems. Since Google
Scholar can't clearly identify these bogus articles, these articles can
cite each other and so build impressive citation counts for the author
or purported author. Algorithms might detect this, but such
detection would be made very much harder by legitimate articles citing
the bogus ones.
There are numerous dangers to this form of academic fraud. One is
that careless researchers may cite these bogus articles and
the data they claim to be based on as a valid way of understanding
Nature. This is an insidious, poisonous, influence on the already
difficult business of scientific research, publishing and
discussion.
Another danger is that citation systems, pre-print servers, search
engines etc. become clogged up with these articles - just as our email
servers have been clogged by spam for decades now.
A further danger is that fake articles, and their authors, may
gain respectability by being cited in genuine articles.
#MA16
Mark Alipio's most cited article
Vitamin
D Supplementation Could Possibly Improve Clinical Outcomes of
Patients Infected with Coronavirus-2019 (COVID-2019)
Mark Alipio
2020-04-08 (Not peer-reviewed.)
Davao Doctors College; University of Southeastern
Philippines
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3571484
Posted: 9 Apr 2020
2020-06-30: 6 citations and 9,886 downloads. This was the 9th
most downloaded coronavirus article on SSRN: SSRN-9th-most-popular.png
Google Scholar (2020-06-30) supposedly 40 citations,
including proper journal articles - but when I checked some, there was
no such citation.
|
2020-07-11 update:
The SSRN page indicates that the
article was revised on 2020-07-10. I downloaded the PDF and found
it is different at the binary level from the CC version mentioned
below. However, the text within the article is identical (using
Beyond Compare). I am not sure
why two different PDF files would have exactly the same creation date,
unless one or both have been modified in some way. Since the text
and the appearance of the pages is identical, I have paid no further
attention to this DD version.
The page now mentions 10,228 downloads, 88,611 abstract views and rank 489.
A complete 2020-07-02 image of the profile page is:
SSRN-MMA-2020-07-02.png . From this the stats for this article:

This is article 16 of the 21 listed below:
#MA-list. See also
#MA-16-critique below.
I have three PDFs of the article. There was at least one earlier
version.
- AA from Grassrootshealth.net
: 151,704 bytes, PDF created 2020-04-15 15:59. local
- BB on 2020-04-23: 149,907 bytes, PDF created 2020-04-23 16:33. local
- CC on 2020-06-24: 157,610 bytes, PDF created 2020-05-07 15:10. local
AA and BB are both "letters" to an editor. CC is not, and has an
abstract. BB completes some instances of "(OH)D" to "25(OH)D" and
adds some +/- figures to the Serum 25(OH)D line of the table.
BB adds the following text which I comment on below:
All
data pertaining to the serum 25(OH)D levels of the cases were extracted
from the onset of symptoms. The hospital conducted serum 25(OH)D test,
along with other clinical tests, every seven days to monitor the status
of patients. For descriptive purposes, mild cases were tested
approximately 3 times, slightly lower compared to original cases (4
times), severe cases (6 times), and critical cases (7 times).
Pre-admission 25(OH)D measured between 7 and 365 days before hospital
admission, was also taken. Mean value for time the latest
pre-admission 25(OH)D level was taken, was 12.65 ± 5.32 days. A total
of 223 cases were originally extracted in the analysis.
To
ascertain no
differences between time points, a repeated measure analysis of
variance (ANOVA) was used and reported no significant differences in
the serum 25(OH)D level of the 212 (95%) cases. Only a small proportion
of cases reported significant differences mainly during the course of
hospitalization. The 212 cases were used for the final analysis and
serum 25(OH)D level taken during the onset of symptoms was considered.
|
CC adds a header at the top of each page:
Note: This
is a pre-print version of the author’s paper before any peer review has
taken.
|
This is technically correct - the article had not been
peer-reviewed. It may
give the impression that the article is to be submitted to peer review
in some unspecified journal - but as far as I know this not occurred.
When I first read this article I assumed the author was doctor.
This seems reasonable since the first of two affiliations is "Davao
Doctors College". In late June 2020 I looked this up and found
the college is attached to Davao Doctors' Hospital, and does not train
doctors.
The main page for the Davao Doctors'
College https://www.davaodoctors.edu.ph/ https://en.wikipedia.org/wiki/Davao_Doctors%27_College
had (2020-06-28) a scrolling slideshow of award winners, including one
for the author who graduated with a Bachelor of Science in Radiologic Technology
2018. On 2020--08-20 the scrolling images of other students remained, but Mark Alipio's was not amongst them.
The author's profile pages are easy to find with web searches.
Some of these might be automatically generated by the web site in
response to his articles:
These are 2020-06-25 snapshots from
Google Scholar of Mark Alipio's articles:
I provide these as a record of my
experience, and no-doubt of others, if they searched for this author as
part of ascertaining the veracity of his articles. A quick
glance shows that this particular article is part of a wider pattern of
publication, albeit - if one actually follows the links - entirely on
preprint servers in 2020. There is an article from previous years
with Mark Alipio as co-author which I did not scrutinise. I am
not suggesting that it is part of the pattern I perceive with these 21
articles in March and April 2020.
Since I am explaining my current understanding of this and other
articles being invalid, it is important to note that I and other people
did not initially think so. I assumed the author was a medical
doctor, probably in his 40s to 60s, conducting vitally needed research
on humanity's most novel and pressing health problem.
A Google search finds multiple instances of "Dr Mark Alipio", though
nowhere does the author present himself in this way. Some
of these instances are in blogs, comments sections of mass media
websites and the like. A few of them are in peer-reviewed
journal articles. For instance:
cites this article:
Moreover,
recently Dr. Alipio has provided substantial information to physicians
and health policymakers. Specifically, it concluded that vitamin D
supplementation improves the clinical course of patients infected with
COVID-19 based on the increased probability of having a mild result
when the serum level of vitamin D increases while a serum decrease in
vitamin D is associated with worse clinical evolution
|
This team of seven presumably highly
qualified researchers and/or clinicians either didn't read or at least misunderstood the article,
which says nothing about observations following vitamin D supplementation.
#MA-list
Mark Alipio's 21 preprint articles generated between 2020-03-22 and 2020-04-27
Articles concerning vitamin D and COVID-19 have their titles and PDF Author text in bold.
The dates here are the PDF creation dates, which can be read from the
Document Properties or similar function of programs such as
PDF-XChange Viewer. So these are the dates on which a Word file was saved as a PDF which was later uploaded to a preprint server.
Some are available on more than one preprint server. So if a PDF
link doesn't work, please try the Google Scholar link instead.
For quick reference I have PNGs named by the article number I assigned.
2020-08-13: Items with a
* have
disappeared.
Title
and link Google Scholar
|
|
Link
1st
page
PNG
|
Date
|
2019-nCOV Scare: Situation Report,
Role of Healthcare Professionals and Clinical Findings
|
GS |
PDF *
01.png
|
3-22
|
Chest
Radiographic Findings of Patients Infected with 2019-nCOV
|
GS |
PDF *
02.png
|
3-26
|
Challenges and Strategies for Curbing
the 2019-nCOV Pandemic: The Case of the Philippines
|
GS |
PDF *
03.png
|
3-27
|
Predicting
Academic Performance of College Freshmen in the Philippines using
Psychological Variables and Expectancy-Value Beliefs to Outcomes-Based
Education: A Path Analysis
|
GS
|
PDF
04.png |
3-27
|
A
Path Analysis Examining the Relationship Between Access Barriers to
Health Services and Healthcare Utilization Among the Publicly Insured:
Insights from a Multiprovince Survey in the Philippines
|
GS |
PDF
05.png
|
3-28
|
A Framework for Predicting Radiologic
Physics Achievement among Radiologic Technology Students
|
GS |
PDF
06.png
|
3-29
|
Structural
Models of Self-Efficacy of Filipino Radiologic Technology Educators,
Current Learners, and Prospective Students in the Senior High School
|
GS |
PDF
07.png
|
3-30
|
Adjustment to college and academic
performance: Insights from Filipino college freshmen in an allied
health science course
|
GS
|
PDF
08.png
|
4-01
|
| Academic
Adjustment and Performance among Filipino Freshmen College Students in
the Health Sciences: Does Senior High School Strand Matter?
|
GS
|
PDF *
09.png
|
4-01
|
Public Policy and Program
Administration in the Philippines: A Critical Discourse
|
GS |
PDF
10.png
|
4-02
|
National Radiologic Technology
Licensure Examination Performance: Predicting Success using
Discriminant Analysis
|
GS
|
PDF
11.png
|
4-07
|
Students' Preferences for Medical
Schools: A Conjoint Analysis
|
GS |
PDF
12.png
|
4-07
|
Academic success as estimated by
locus of control and motivation
See #MA13-similar.
|
GS |
PDF
13.png
|
4-07
|
| Epidemiology and Clinical
Characteristics of 50 Death Cases with COVID-2019 in the Philippines: A
Retrospective Review |
GS |
PDF *
14a.png
14b.png
|
4-08
|
A
Structural Model of Organizational Commitment among Higher Education
Economics Educators
|
GS |
PDF
15.png
|
4-08
|
Vitamin D Supplementation Could
Possibly Improve Clinical Outcomes of Patients Infected with
Coronavirus-2019 (COVID-19)
|
GS |
PDF *
16a.png
16b.png
|
4-09 |
Do latitude and ozone concentration
predict Covid-2019 cases in 34 countries?
|
GS |
PDF
17a.png
17b.png
|
4-10 |
Do Socio-Economic Indicators
Associate with COVID-2019 Cases? Findings from a Philippine Study
|
GS |
PDF *
18a.png
18b.png
|
4-11 |
Determinants of tuberculosis
incidence in East Asia and Pacific: A panel regression analysis
|
GS |
PDF
19a.png
19b.png
|
4-15
|
Revenue
Administration in the Philippines: Significant Collection
Reforms, TRAIN Law, Fiscal Incentives, Excise Tax, and Rice
Tariffication Law
|
GS |
PDF
20.png
|
4-15
|
Education during COVID-19 era: Are
learners in a less-economically developed country ready for e-learning?
|
GS |
PDF *
21.png
|
4-27 |
Article 16 is the one I am
most concerned with - see above:
#MA16. I listed its date as April 09 =
4-09,
since this is the date of posting on
SSRN
. The PDFs I have of various versions are of later dates,
as mentioned above.
Terse critiques of 21 articles by Mark Alipio
Since
some of the articles mention journal names, it is important to check to
what extent the article is in fact associated with such journals.
2020-08-13: Items with a
* have
disappeared.
Start
of title
|
Link
1st
page
PNG
|
My
terse description of the article
|
2019-nCOV Scare: Situation Report,
Role of Healthcare Professionals and Clinical Findings
|
PDF *
01.png
|
General discussion of public
data.
Header is
for the International
Journal of Multidisciplinary Health Sciences Research. There
is no such journal. The two websites I found entitled International
Journal of Multidisciplinary Health Sciences
are both defunct. The issue number 10 exceeds the number of
issues per year, which is 4, for the journal which was most recently
active.
There are 46 SARS-CoV and SARS-CoV-2 references but none of them are
mentioned in the text.
|
| Chest
Radiographic Findings of Patients Infected with 2019-nCOV |
PDF *
local
02.png
|
General discussion of public
data.
Header as
above.
There are 53 references, none of which are mentioned in the text.
Most are to COVID-19 articles but 10 are to articles for whom this author is listed as the sole or co-author
This
looks like an attempt to manipulate Google Scholar and other citation
systems.
|
| Challenges
and Strategies for Curbing the 2019-nCOV Pandemic: The Case of the
Philippines |
PDF *
local
03.png
|
General discussion of public
data.
The
final two references are to the above articles, but are not mentioned
in the text.
This
looks like an attempt to manipulate Google Scholar and other
citation systems.
|
Predicting
Academic Performance
|
PDF
04.png |
Analysis of results from vaguely
defined survey of 12,453
students in 70 higher education institutions.
|
A
Path Analysis Examining
|
PDF
05.png
|
Analysis of results from vaguely defined
survey of 7,234
Filipino residents using multi-stage cluster sampling.
|
A Framework for Predicting
|
PDF
06.png
|
Analysis of results from vaguely defined
survey of 954 Radiology
Physics students randomly selected from 12
Radiologic Technology schools in the Philippines.
|
Structural
Models of Self-Efficacy
|
PDF
07.png
|
Analysis of results from vaguely defined
survey of 256
Radiologic Technology educators and 2,451
students randomly selected from 22 Radiologic
Technology schools in the Philippines. Also 4,263 prospective
Radiologic Technology students from the 30 senior high schools of the
Philippines. This seems rather low for a country of 100
million people.
|
Adjustment to college
|
PDF
08.png
|
Analysis
of results from survey in June to October 2018 of 132 first year
Radiologic Technology students in an unspecified higher education
institution in the Philippines, who were chosen through stratified
random sampling. This would require the total number of students
to be multiple times larger than this, which seems like a rather large
number for any one institution given there are either 12 or 22 Radiologic
Technology schools in the Philippines. I thought this was a lot
of such schools, but there are
102.
There is
no information on the number of students from which the respondents
were chosen, how they were assigned to groups for the purpose of
stratified random sampling, the statistical goals of the survey, or how
Slovin's formula was used to guide these choice of which students to
include in the survey.
There is
no record of the questions or of the answers - just analysis of the
answers.
|
| Academic
Adjustment and Performance
|
PDF *
09.png
|
Analysis of results from vaguely defined
survey of 14,062
participants in different health science disciplines at 79 higher
education institutions (HEIs) in the Philippines.
|
Public Policy and Program
|
PDF
10.png
|
General discussion. Some
sentences may not have been written by a human:
The
Identity Crisis should be viewed
from the perspective of development administration or from a field now
called Development Public Administration.
Develop research programs that focuses on the problems in the country,
looking into the behavioral
insurance of politics and administration, and the accompanying features
that open the government to
development process.
Five
irrelevant references to articles by the same author are not mentioned in the text.
This
looks like an attempt to manipulate Google and other systems which count
citations.
|
National Radiologic Technology
|
PDF
11.png
|
Analysis of results from vaguely defined
survey of 2,036
graduates of a baccalaureate Radiologic Technology program in 2016,
2017, and 2018 from 24 higher
education institutions (HEIs) in the Philippines.
This
is the first study to discriminate
passing
from failing graduates in the national RT licensure examination based
on the selected predictor variables and the astounding
precision of classifying graduates is a remarkable result for HEIs
included in the analysis.
|
Students' Preferences for Medical
|
PDF
12.png
|
Analysis of results from vaguely defined
survey of an unspecified number
of respondents selected from 24,263 prospective students in the
health sciences and medical courses from the 125 senior high schools in the
Philippines.
Multi-stage
cluster sampling technique was used to recruit the sample. A face to
face interview with a set of stimulus cards or through a
self-completion questionnaire was used to collect the data and Adaptive
Conjoint Analysis (ACA) was performed to analyze students’ preferences.
|
Academic success as estimated
|
PDF
13.png
|
Analysis of results from vaguely defined
online survey of 21,012
freshmen.
A
descriptive-correlational study using online survey questionnaires
was employed to 21,012 respondents who were chosen through simple
random sampling and Slovin’s formula.
See #MA13-similar.
|
Epidemiology and clinical characteristics
of 50 death cases with Covid-2019 in the Philippines: A retrospective
review
|
PDF *
14a.png
14b.png
|
Brief analysis of 50 COVID-19
deaths from 2020-01-30 to 2020-04-03. However, I
can't see that the patient details are actually publicly available
sites as claimed. No details of how these 50 cases were chosen
from the 135 deaths in this period (https://endcov.ph/dashboard/)
|
A
Structural Model of
|
PDF
15.png
|
Analysis of results from vaguely defined
survey of 871 higher
education Economics educators.
The
author names of its 28
references all start with A or B. Except for those attributed to this author, none of them are
mentioned in the text.
|
Vitamin
D supplementation could possibly improve clinical outcomes of patients
infected with Coronavirus-2019 (COVID-2019)
|
PDF
16a.png
16b.png
|
Analysis of results from vaguely defined data
extraction from vaguely defined hospitals:
Using
the database of three hospitals in Southern Asian countries, a
retrospective multicentre study of 212 cases with laboratory-confirmed
infection of SARS-CoV-2 was conducted.
See further notes below.
|
| Do
latitude and ozone concentration predict Covid-2019 cases in 34
countries? |
PDF
17a.png
17b.png
|
Analysis
of number of cases of COVID-19 in 34 countries with respect to upper
atmosphere ozone. The ozone data is reproduced and looks
realistic, though there is little variation between them - I calculated
334 average and SD 47.
The
number of cases in the countries is not listed. The analysis is
meaningless because no account is taken of the population of each
country.
|
Do
Socio-Economic Indicators Associate with COVID-2019 Cases? Findings
from a Philippine Study
|
PDF *
18a.png
18b.png
|
Analysis of number of cases of
COVID-19 in 17 regions of Philippines. Case number data is
presented but not
the 7 items of socioeconomic data for each region.
The analysis is meaningless because no account is taken of the
population of each region, which varies by a factor of 8.2. |
Determinants of tuberculosis
|
PDF
19a.png
19b.png
|
Analysis of TB incidence per
100,000 people and various socioeconomic variables for 23
countries.
The
analysis is meaningless because the countries are not
listed and no data is presented.
|
Revenue
Administration
|
PDF
20.png
|
Cursory
discussion of public data. The first reference is not referred to
in the text. Neither are the other five, which are all to articles in this list of 21 - none of which are relevant to this
article.
This
looks like an attempt to manipulate Google and other systems which count
citations.
|
Education during COVID-19
|
PDF *
21.png
|
2000
students were sent an email survey. Educational involvement,
geographic location and other selection criteria were not defined and
they were supposedly initially contacted via Facebook, Twitter
and other social networking sites. However, these sites
do not provide email addresses.
440 responded. This seems like an extraordinarily high rate
considering the 27 questions plus demographic details.
The 27 questions were adapted from a cited source
which allowed responses on a 1 to 5 scale. In this supposed
survey, answers were Yes/No and all 440 respondents responded Yes or
No, with none recorded as not responding to a question. It is
impossible to imagine this 100% response rate if they responded via
email. The email questionnaire is not reproduced.
The questions were shown not in the original order, but in order of
decreasing Yes response. The
percentage of Yes answers varied very little between the questions -
from 45.5 to 44.0 - so this data is obviously fictitious.
|
This article filled a gaping hole in vitamin D and COVID-19 research
I initially accepted this article 16 as
genuine. It was the first article I knew of which showed
what I and many other people expected: a correlation between disease
severity and low vitamin D 25OHD levels. While infection is
sometimes thought to lower vitamin D levels, I think the evidence for
this is limited. So, assuming that this could account for only a
small part of the association, it is reasonable to conclude that the
causation flows the other way: from low vitamin D to worse outcomes.
There are numerous reasons to believe that low vitamin D would cause
this directly. However, other causality pathways also need to be
considered, such as low vitamin D causing other conditions, over a long
period of time, and those conditions causing worse outcomes.
Also, those conditions might cause both low vitamin D and worse
outcomes for COVID-19.
Despite the causation of severe symptoms not necessarily being directly
and entirely due to low vitamin D levels, I think it is reasonable to
assume that a great deal of causality is by this pathway, which raises
the possibility of preventing or reducing these symptoms and resultant
damage and death by vitamin D supplementation.
With the world in the early stages of the COVID-19 pandemic, with more
and more worrying reports of death, and serious harm to the brain,
lungs, heart and other organs, the thought that a few milligrams of
inexpensive (USD$2.50 a gram in 1kg lots ex-factory) vitamin D (4000IU
a day is 0.1mg) might prevent such tragic and disastrous harm and death
motivated me and many others to search for evidence this would be true.
This article, soon joined by the Indonesian article, is what we wanted
and needed in our urgent attempts at raising awareness among doctors,
researchers and the public. So, in a hurry (I certainly
was) many of us took what we wanted from the article - the numbers of
patients in different classes of vitamin D deficiency and
symptomatology - and made our own tables and graphs, telling everyone
we could about it.
It never occurred to me that someone would write an entirely
fictional
research article and publish it in any form as if it was a genuine
report of real observations. I assumed the results were
from a medical doctor, working in the Philippines, under difficult
early stage pandemic conditions. I didn't scrutinise the article
for weaknesses or inconsistencies.
There is no sign of the article being humorous, or a send-up. It
is a quickly written document which shows the author has a non-trivial
understanding of vitamin D, the immune system and COVID-19 - well
before such notions were more widely discussed. Indeed, if
most doctors had had such an understanding, they would have long been
advocating that
everyone
robustly supplement with vitamin D to raise their 25OHD levels to the
40 to 60ng/ml range which experts have been recommending since 2008:
https://www.grassrootshealth.net/project/our-scientists/
So I think the author knew more about vitamin D than some
or many doctors.
Shortcomings of the MA16 article itself
These shortcomings of the article are
mainly ones I noticed once I began to suspect its veracity.
My initial impression was that this was the work of a doctor somewhere
in the Philippines who had access to the records system of hospitals
and had taken some precious time to analyse 250HD tests which had
already been done. I was pleasantly surprised that hospitals in
this developing nation were suitably aware of vitamin D deficiency in
general to be doing these tests.
I remember wondering about the 25OHD tests which were done before
COVID-19 infection. I guessed that these tests were part of
ongoing surveillance of outpatients or something like this.
I also wondered about the extensive nature of these tests across three
hospitals.
However, I didn't think too much about the details because the data
reflected what I suspected was the case - higher proportions of severe
symptoms with lower 25OHD levels.
I should have been wary of this statement:
Using the database of
three hospitals in Southern Asian countries,
|
Why would there be one database for multiple hospitals in multiple
countries? Was this a typo and the author meant
"databases"? I cut the author some slack at the time,
being from a developing nation, in a time of crisis - no-doubt working
under great difficulties.
Why weren't the countries mentioned? They should be.
Perhaps the author did not have proper authority to access this data,
but did so anyway. It is a time of crisis after all, and who
knows what dodgy security was in place and what bureaucracy which might have
stood in the way of this important work.
I think I first read the BB version of the article, not knowing there
had been an earlier version without the following text:
All
data pertaining to the serum 25(OH)D levels of the cases were extracted
from the onset of symptoms. The hospital conducted serum 25(OH)D test,
along with other clinical tests, every seven days to monitor the status
of patients. For descriptive purposes, mild cases were tested
approximately 3 times, slightly lower compared to original cases (4
times), severe cases (6 times), and critical cases (7 times).
Pre-admission 25(OH)D measured between 7 and 365 days before hospital
admission, was also taken. Mean value for time the latest
pre-admission 25(OH)D level was taken, was 12.65 ± 5.32 days. A total
of 223 cases were originally extracted in the analysis.
To
ascertain no
differences between time points, a repeated measure analysis of
variance (ANOVA) was used and reported no significant differences in
the serum 25(OH)D level of the 212 (95%) cases. Only a small proportion
of cases reported significant differences mainly during the course of
hospitalization. The 212 cases were used for the final analysis and
serum 25(OH)D level taken during the onset of symptoms was considered.
|
There are lots of clangers
here. If the version I read then had this text, I
should have paid much more attention.
Why would patients be tested fixed numbers of times depending on
severity. Severity varies over time and some die or are
discharged before others. 7 weekly measurements for severe
symptom patients makes no sense, because some would have died by then,
and because this would have had to be in February and March, when there
were few cases outside China.
I remember wondering why there were one or more 25OHD tests taken
before the onset of COVID-19, up to a year before. I glossed over
this concern - imagining some kind of outpatient monitoring
arrangement, which I thought both unlikely and actually quite
impressive, considering the lack of interest many doctors in first
world countries have in vitamin D. I really should have
questioned the veracity of the whole article for this and other reasons.
Then there is the question of three separate hospitals doing similar
25OHD tests on outpatients when they were not even in the same
country. I probably thought about this for a few seconds
before moving on, provisionally impressed by the foresight of these
doctors in countries far less rich than my own.
This reminds me of the pattern of spam from African countries - or at
least ostensibly from them. No-one would believe an email
from a previously unheard-of person from Germany, the UK, Japan or the
USA who suddenly was considering donating a few million dollars , or
was urgently in need of a place to park his or her vast fortune due to
some impending coup, assassination plot or whatever. But
one can imagine such quasi-noble characters bumbling through their
troubles, burdened by their immense and probably ill-gotten wealth,
struggling with English, legality and morality if they came from some
distant African country with immense oil or mineral wealth. The effect is to cut the spammer some extra slack due to their
non-English-speaking and generally third-world background.
I should have recognised that the whole article was made up, with the extreme
precision of the following, and there being no reason at all for the
pre-admission 25OHD tests so soon before:
Mean value
for time the latest
pre-admission 25(OH)D level was taken, was 12.65 ± 5.32 days.
|
This would require doctors in all three hospitals, in different
countries, to either be doing these frequent 25OHD tests to a vast
number of people who were not ill at the time, or only for the smaller number of people who
would soon get COVID-19 - without a time machine to predict this.
What were the significant differences in these multiple pre-illness
25OHD levels? What was the criteria for exclusion from the subset
chosen for the main analysis?
If I had known that these paragraphs had been added after the initial
version of the article, I might - should at least - have been more
suspicious. However, I had no idea some people were writing
entirely fictional research articles.
Frequency
and percentage were used for categorical variables.
|
Never having studied statistics, I usually gloss over these parts of
research articles - but what does this actually mean in this
context? I still have no idea.
Also, I didn't notice this:
. .
. nature of the study and open-access
data used
|
If I had recognised that the data was open-access, I would have expected its
URL to be mentioned. I would probably have written to the author, though I was sure he was very busy, to request access
to such data so I could scrutinise it in greater detail than he had
reported it.
My eyes went straight to the 25OHD levels in table 1. Not so much
the averages but the number of patients in each of the three bands of
values for the four levels of severity.
I wrote this up as a table to make it really easy for people to see the
great dependence of severity on vitamin D levels:
25OHD
All Mild Ordinary Severe Critical
ng/ml
>
30 55 47
4
2
2
20-30
80 1
35
23
21
<
20 77 1
20
31
25
While I think the real author is to be congratulated for
having an early sense of the degree to which low 25OHD levels probably
cause COVID-19 disease severity, I think he was straining
credulity somewhat with the sharp dichotomy between severity above and
below 30ng/ml. My best guess, in July 2020, is that
the relationship is not as sharp as this - since we are dealing with
biological systems with numerous dimensions of variation from one
individual to another.
I took no interest in the predictions the author had supposedly
discovered - in part because I lack the statistical knowledge to
understand what was supposedly being achieved there. I could have
educated myself on this quick-smart if I was interested - but what I
really wanted was the observational data.
Until now I didn't notice the final sentence, which is a clanger:
In this
case, Vitamin D supplementation may play an important role to raise
1,25-dihydroxyvitamin
D [1,25(OH)2D], the biologically active form of Vitamin D in the blood.
|
The immune system is generally not dependent on the serum 1,25OHD
levels. Anyway, these are generally reasonably stable, for a
reasonably wide range of D3 inputs and so 25OHD levels. What the
immune system requires for proper operation is robust levels of 25OHD -
I now
know that 40 to 60ng/ml is recommended by many researchers and a few
doctors, and this is directly affected by supplementation levels.
Still, I could imagine someone collecting these statistics while not
having a very detailed understanding of how vitamin D affects the
immune system.
I don't recall using Google to search for the author. I pictured someone in their 40s to 60s, with a wealth of
experience, and a busy caseload, taking some time to access and analyse
some crucial and so-far unreported data.
I tended to think of him treating COVID-19 patients, and was vaguely
expecting further articles on the effectiveness of the vitamin D
supplements suggested in this article.
An Indonesian article from five authors with no publication history
Important update 2020-07-27:
See the following article in which three Indonesian MDs find no trace
of the purported authors of the above article. This includes searching
the Indonesian Medical Council database and contacting the hospital
mentioned in the article:
This is the first of two fake articles
which fall into the pattern established by Mark Alipio's articles, with
which they share many commonalities. The other is the "Glicio"
article mentioned below:
#G-critique
"Raharusuna" (in both PDF versions I have seen) seems to be a typo
since Google only finds it in pages which mention this article.
The article was posted to the SSRN preprint system at this URL.
The page where it was listed disappeared sometime around mid-to-late
June 2020. I don't have
a snapshot of what the page looked like, but I found an image
EbEe6w_U0AAzSI1.png apparently of this
page, in this
tweet
. It shows the initial date for the article is 30 April.
I have a PDF I saved from
this page on 2020-05-02.
This page, which seems to be associated with SSRN, tracks websites,
social media etc. which mention the article:
Here is a screenshot of that page from 2020-06-30:
plu~mx~ssrn~a~ssrn_id~3585561.png
. You can see the first author's surname is spelt
Raharusuna while the article was
listed with this name spelt
Raharusun.
SSRN is owned by Elsevier so this page indicates the article is
published by Elsevier.
The date in the text of the file is April 26, 2020.
Here are the versions I am aware of. "RR", "SS" and "TT" are my names.
- RR I downloaded from SSRN. 148,019 bytes, PDF creation date
2020-04-26 19:12. This would be the original version. It
was the only one I was
familiar with until 2020-05-30 when I searched for PDFs of the article
and found:
- SS I found at: https://emerginnova.com/patterns-of-covid19-mortality-and-vitamin-d-an-indonesian-study/
and downloaded on 2020-06-30. 211,568 bytes, PDF creation date 2020-05-06 10:59.
- TT is a modified version, not from SSRN, with an extra page at
the start, apparently created by Lorenz Borsche and Dr. Bernd Glauner,
June 2020. This is available from: https://borsche.de/res/Patterns_of_COVID_19_Mortality_and_Vitamin_D_An_Indonesian_Study.pdf
I downloaded a copy on 2020-06-30. It is 629,563 bytes. Except for
the new first page, it is identical to SS. It has the same PDF
creation date and PDF Author. The PDF Producer field has been
changed from the original "Microsoft ® Word 2019" to something which
indicates the file was created by software from https://www.pdf-tools.com
. I will not discuss the first page in this section, but in the next section I discuss a graph from this first page.
So two versions concern us: RR is the original and SS is an update 10
days later. SS has two extra elements. Firstly, at the end
of the Descriptive Statistics section, there is a new paragraph:
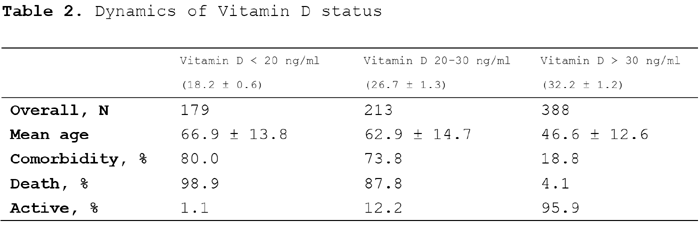
A
total of 179 cases had Vitamin D deficiency (Vitamin D < 20 ng/ml),
mean level of serum 25(OH)D and mean age for this group were 18.2 ± 0.6
ng/ml and 66.9 ± 13.8 years, respectively (Table 2). 213 cases had
Vitamin D insufficiency (Vitamin D 20-30 ng/ml), mean level of serum
25(OH)D and mean age for this group were 26.7 ± 1.3 ng/ml and 62.9 ±
14.7 years, respectively. 388 cases had normal Vitamin D levels
(Vitamin D > 30 ng/ml), mean level of serum 25(OH)D and mean age for
this group were 32.2 ± 1.2 ng/ml and 46.6 ± 12.6 years, respectively.
80.0% of Vitamin D deficient cases had pre-existing conditions
(comorbidity). 73.8% of Vitamin D insufficient cases had pre-existing
conditions (comorbidity). 18.8% of cases with normal Vitamin D levels
had pre-existing conditions (comorbidity). 98.9% of Vitamin D deficient
cases died while only 1.1% of them were active cases. 87.8% of Vitamin
D insufficient cases died while only 12.2% of them were active cases.
Only 4.1% of cases with normal Vitamin D levels died while 95.9% of
them were active cases.
|
Secondly, there is an additional table, though the text references to the prior tables
2 and 3 were not bumped to 3 and 4:
This page no longer contains anything about my attempts to find out
about the authors. However, here are some notes about the
hospital mentioned in the paper. I only pursued this in late
June, once I was evaluating my hypothesis that the article does not
report on real research.
Before that, I assumed that one, some or all authors worked at a
hospital somewhere in Indonesia - and I was aware that it was not on
Java or Sumatra, but on the less densely populated Kalimantan district,
which is part of Borneo. The address is:
RSUD Kabupaten SukamaraKec. Sukamara, Kabupaten Sukamara,Kalimantan Tengah 74171, Indonesia
RSUD Kabupaten Sukamara translates to
Sukamara
District Hospital.
2020-08-13 update:
Some of the text below is now in grey since I wrote it on the
assumption that the website I was looking at was the hospital's
website. As explained in the #indon-govt section below, I now know that website was fake. The hospital does not and never had a website.
I
initially assumed it was like a major public hospital in Australia
or other developed countries - hundreds of beds, well connected as part
of a larger presumably government network and with all aspects of its
operation fully certified. I didn't look up the location on
Google maps until about 10th July (link). It is a small hospital, in a semi-rural location, 3km south of the
centre of Sukamura. (In 2019, 63.5 percent of 2,813 hospitals in Indonesia were run by private organizations.) Sukamara
is the capital of Sukamara Regency [W]
which in 2014 had a population of 48,134 in its 3,827 square
kilometres. There are no Google streetview pictures, which is not
surprising. The two-storey hospital is located in some streets
which are not part of Google Maps' database. Its opening hours
are 6AM to 6PM Monday to Saturday.
Its website http://rsudsukamarakab.net (on 2020-07-11) has its two most recent updates in April. Searching for web pages which mention or link to rsudsukamarakab.net
(with English and Indonesian selected in Google's settings), I found
only pages which list domain names and a handful of Facebook
pages. I found it surprising that any hospital, even a small one
in a rural area, would have so few links to its website. However,
on 2020-08-13, this makes sense, because the website I was viewing,
which disappeared sometime around mid-July, was fake.
According to 2012 Worldbank data cited in Wikipedia there were 0.2 physicians and 1.2 nurses per 1000 population. I couldn't find a list of hospitals at https://www.kemkes.go.id . The hospital is presumably accredited, though in early 2019 it apparently was not .
If
I had looked up this hospital in April or early May when I first read
and cited this article, I would have found it to be very different to
what I imagined. Then, I might have paid greater attention to
potential weaknesses in the article.
Looking up the institution(s) the authors are affiliated with is an
important part of assessing the veracity of an article. I
just assumed that hospitals in remote areas of Indonesia were operating
on the same scale and with the same level of expertise as the larger
hospitals here in Australia - although I guess they might be
smaller.
It is possible that a
doctor
living in this area could communicate with large government hospitals
in the rest of the country, working with three colleagues, to obtain
all the required data, analyse it and collectively write the Word file
from which the PDF file was created, in about a day and a half from the
end of data collection - as I found in July 2020 would have to be the
case given the article's date range for data collection and the PDF
creation date less than two days after this.
The content of the Indonesian article
This article fits the pattern I
observed in many of the Mark Alipio articles: a vaguely defined survey
or set of sourced data, with no actual raw data - just some analysis
and discussion.
The first version PDF was made at 7:12PM on 26th April, yet the article
states that the researchers used electronic medical record data from March 2 to
April 24. I can't imagine this being realistic. Blood tests
etc. take time to perform and to enter into data systems. How
could the researchers perform their analysis and write their article in
a day or so? This is a clanger I should have noticed.
Again we see vague descriptions of the data sources: "Indonesian
government hospitals". "To ensure anonymity, all names were
preserved throughout the analysis." makes no sense.
I should have paid more attention to problems such as this:
The
pre-admission serum 25(OH)D levels were considered for the analysis.
Serum 25(OH)D level was checked by two physicians based on the
available clinical data of the patients.
|
Why had all these 780 patients been tested for vitamin D levels before
being admitted to hospital? "considered"? Why would two
physicians be needed to establish a patient's 25OHD level if it had
been recorded? Who were these physicians - and how did they do
this in a fraction of a day, for a data dump of 780 patient
records? What about incomplete data?
There are a number of similarities between the Mark Alipio article 16 (A16)
and this Indonesian article (R1). Both have a unique (in
the entire world, according to Google) header at the top of each page.
A16
|
R1
|
Note: This is a pre-print
version of the author’s paper before any peer review has taken.
|
Disclaimer: This is a
preliminary study for early dissemination of results. Data are subject
to changes
|
Header was not present on the BB version PDF date 2020-04-23 but was added with the CC version, PDF date 2020-05-07.
|
Header was not present on the RR version PDF date 2020-04-26 but was added with the SS version, PDF date 2020-05-06. |
I don't understand what the first phrase in the following table means -
it is quite rare.
A16
|
R1
|
Frequency and percentage were
used for categorical variables. (2,000 Google hits.)
|
frequency and percentage were
employed for categorical variables. (2 Google hits.)
|
I don't have time to pick through the
minutiae of the data and analysis.
One thing which did strike me as curious when I first read it, and
which remains a problem, is the extreme sharpness of the relationship
between 25OHD level and death. I wrote it up as:
25OHD
Death rate
ng/ml
>
30 4.2%
20-30
49.1%
<
20 46.7%
There is further analysis, supposedly based on the data of this article,
at:
https://borsche.de/res/Indo_3_EN.pdf
which
I don't have the time or inclination to check. This
analysis is stated to have been done by or in collaboration with the
statistician member of the author team. According to the
next PDF, this collaboration resulted in the graph presented in the new
first page of:
https://borsche.de/res/Patterns_of_COVID_19_Mortality_and_Vitamin_D_An_Indonesian_Study.pdf
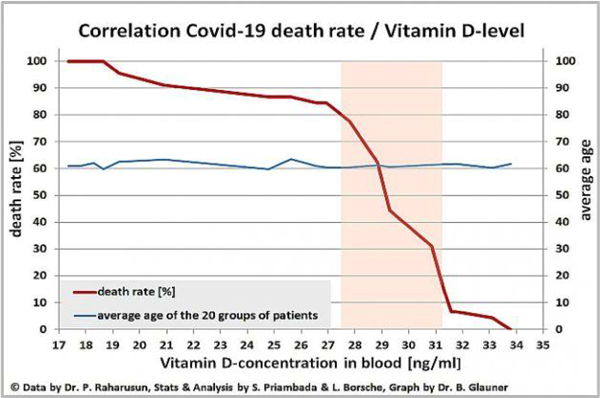
This is so sharp. I should have paid more attention to this when
I first reproduced the graph on my site. A 20% drop in 25OHD
levels leads to the death rate going from a few percent to 80%??
This is surely not real data. Even if a population of humans
responded in this dramatic and clear-cut manner to a slight change in
25OHD levels, the per-sample errors in the 25OHD measurements would preclude
such a sharp relationship appearing in the data. I really should
have thought more about this before taking this data seriously.
I find this data unbelievable. However, I have no formal
qualifications in any field, and I hope other people will make up their
own minds about this, and the other aspects of the article.
Important update 2020-08-03: I
have been corresponding with Dr Raymond Pranata, who is one of three
authors of the article previously mentioned in which they report
finding no trace of the 'Raharusun" article's authors, and list several
critiques of its veracity:
COVID-19 and Misinformation: How an Infodemic Fueled the prominence of Vitamin D
Joshua Henrina, Michael Anthonius Lim and Raymond Pranata
British Journal of Nutrition 2020-07-27
https://doi.org/10.1017/S0007114520002950
|
Dr Pranata kindly authorised me to reproduce here three further reasons
why he and his coauthors doubt the veracity of the "Raharusun" article:
1)
Badan Penyelenggara Jaminan Sosial (BPJS) has a reimbursement cap,
ordering tests should consider the budget. Only essential examinations
can be ordered or the expense will exceed the reimbursement cap. Thus,
Vitamin D is not regularly checked in the hospital; unless of course if
there is indication, i.e: rickets, osteoporosis, etc. Since the study
is retrospective in nature, it is unlikely that they have Vitamin D
data on 380 deaths over 647 on their study period.
2)
The second one is pretty obvious, up until now, there were only 2
confirmed cases of COVID-19 in RSUD Kabupaten Sukamara, and around 90
deaths in Central Kalimantan Province. So, the data has to be taken
from large hospitals in big cities. These hospitals include Rumah Sakit
Cipto Mangunkusumo Fakultas Kedokteran Universitas Indonesia (RSCM)
(National Referral Hospital), and RS Gatot Subroto (Central Army
Hospital), RSPI Soelianti Soeroso (National Referral Center for
Infectious Diseases), and RS Persahabatan (National Referral Center for
Respiratory Diseases). They have to at least acknowledge these
hospitals and add co-authors. By the way RSUD Kabupaten Sukamara is not
a COVID-19 regional referral hospital. Since they are not willing to
list the name of the hospitals (like SurgiSphere scandal), the data is
most likely fabricated.
3)
The third one supports the second point, it is impossible to get that
many patients unless you collaborate with multiple centers in Jakarta
at that time. Even now, there were only around 90 deaths in Central
Kalimantan and ZERO deaths due to COVID-19 in RSUD Kabupaten Sukamara.
|
Also, despite the Campaign Owner (Lorenz Borsche) being fully aware of these criticisms
and the article by the three doctors - as discussed in acrimonious
email correspondence I have been a party to since 2020-07-28 - this
fundraiser for COVID-19 research, in honour of the late "Dr Prabowo
Raharusun", to be administered by Mark Alipio and "Dr Glicio" (below),
remained active until it stopped accepting donations on 2020-08-16:
Here is a composite screenshot of the fundraiser page on
2020-08-05. It remained in much the same state, with the image of
the supposed gravestone, until 2022-08-16 when two more small donations
had been made and no more were accepted.
Update 2020-08-20:
There was a major change to the fundraiser page. The gravestone
photo was removed and the state of the page was as shown in this PDF,
pages 6 to 9 of which reflected the state before this update:
It seems that Lorenz Borsch is contemplating several scenarios in which
the whole affair was a scam (and so in which he was a dupe, and
unreasonably denied the veracity of my efforts, and those of Dr Pranata
and colleagues, to help him). Yet he does not seem to really
believe any of these scenarios, since he refers to us as "attackers
from AU and Inonesia". He notes that the "graveplate" image might
have been photoshopped, offers to repay all donations and notes that
this will not put him in financial trouble. The graph is still
there.
#academic-rot
Important update 2020-08-20:
Academic rot as these fraudulent articles continue to be cited in
perfectly good websites and academic journal articles
There were a number of people - mainly
in the UK and Germany, but with some in the USA - who had engaged in
extensive email correspondence and at least one phone call with persons
they believed to "Dr Raharusun" and at least one of his
co-authors. Monies were solicited from and donated by some
of these people for supposed hospital expenses. Offers were made
of vitamin D3 supplements to be sent to Indonesia to further research,
but these were not accepted. Further data was requested from the
supposed Raharusun study but only one person received anything in this
regard - or at least correspondence regarding further analysis of such
purported data - and that person did not share it with anyone
else. Then there was the fundraiser mentioned above.
Further data was also solicited from Mark Alipio and at least one
larger, different, "data" set was provided. I haven't seen this,
but some people who received it quickly decided it was fake, due to
gaps in the distribution of data points which would never occur in real clinical observations.
Some of these people (I know this from email correspondence with
multiple former believers) became suspicious in the early stages of
affair, I think around May. Others retained their belief in the
veracity of the "Raharusun" article and in the existence of its
purported authors, and likewise of the veracity of Mark Alipio's
best-known article, MA16 above until they became aware of the critiques
on this webpage. As far as I know, most of
the remaining believers have now (2020-08-20) - 7 weeks after this page
was first first established and made known to them - totally or almost
totally abandoned their former beliefs. The first news I had of
Lorenz Borsch having any doubts about the veracity of the "Raharusun"
article was on 2020-08-20, as described
above.
With the three most important articles now withdrawn from their
preprint servers - ("Raharusun", then "Glicio" and in recent days Mark
Alipio's most widely cited MA16 article (see list above) - there should
be absolutely no reason to cite these articles in any website, journal
article etc. except to note that these fake articles have been
withdrawn, and ideally to point to this page, the Henrina et al, article
cited above, and the hospital director's statement mentioned below, as evidence that these
articles were fraudulently created.
However, these articles and the derivative work (graph above) supposedly based on
analysis of the supposed data of the "Raharusun" article, have been
cited in legitimate journal articles and probably will continue to be
cited in the future. These articles are a cancerous
development, and to the extent that author C cites them because he or
she saw them cited in an article by author A or B, without checking that the
article is still available, and is not fake, then these articles
arguably constitute a viral infection or some other pathological species
of self-propagating academic fraud.
Ideally I would list all such articles here, and write to all their
authors. I don't have time for this. If someone would search for
such articles on
Google Scholar and do this for at least some of them and let me know, I would really appreciate it.
Here, I want to point out a prominent and in many ways
promising new
website regarding vitamin D which cites the bogus graph developed by
Lorenz Borsche and Dr Glauner, supposedly from the "Raharusun data" as
mentioned in the previous section.
The site is:
It is produced by the
Organic & Natural Health Association https://organicandnatural.org/about-us/mission-and-vision/
whose
membership
consists of some nutrition organisations (and one concerned with
grassfeed meat certification) and quite a number of nutrition
supplement companies.
There's an image of a cheery and apparently very healthy brown-skinned
young woman with the caption "My level is 55! What's
yours?". Assuming this is ng/ml (nmol/L would be
only 22ng/ml) then this is a perfectly healthy 25OHD level. I
am very glad to see vitamin D supplementation promoted, including with
the prominent mention of
Ken Redcross MD https://www.drkenredcross.com
, who also has a line of nutritional supplements, including this one,
which combines a gram of EPA/DHA omega 3 fatty acids (which would
normally only be found in several grams of fish oil) with 0.05mg
(2000IU) vitamin D3 and 250mg vitamin C:
I think this is an unusually good dietary supplement and I think the website is an
excellent development, with its focus on people with pigmented skin and the elderly who are most at risk of vitamin D deficiency.
Here is Dr Ken Redcross
tweeting (2020-08-18) about his new website
PowerOfD.org :
For the avoidance of doubt:
I totally support the aims of this website. My
criticisms of their use of the bogus data are not directed at Dr Ken
Redcross or any of the other MDs and other specialists who are behind
this website:
I salute these energetic people for developing this website.
The other reason I mention them is to demonstrate that good,
professional, people can easily be swept into the process of believing,
making healthcare decisions based upon, citing and so promoting and
further propagating bogus research. It has probably not occurred
to them that anyone fake such research articles. It didn't occur
to me until late June, and that was only prompted by the suspicious
supposed death of a supposed author. I had been citing these
articles with enthusiasm and even gratitude (to
Dr Alipio in the Philippines for doing much-needed vitamin D research in the midst of the COVID-19 pandemic), simply because it had no occurred to me anyone would fake research articles like this
and because the article presented data which confirmed my belief that low vitamin D was driving COVID-19 severity
and because there was a lack of such research.
The main page of
PowerOfD.org
has 10 boxes concerning vitamin D and depression, sleep,
healthier children etc. each with a link to another website and a
research article. I assume these are all good.
Then there is a link to a page with a video of Joseph Mercola
interviewing Ken Redcross. More on that in a moment.
Below this are more links to research articles and then this black
white and orange graphic, boldly captioned:
STATS DON'T LIE
Actually, statistics need to be interpreted very carefully at the best of times. In this case, everything in the graph is
fake.
See the previous section for the image from which this was adapted and
why the data is not just fake, but wildly unrealistic. Please
also see all the research linked to from
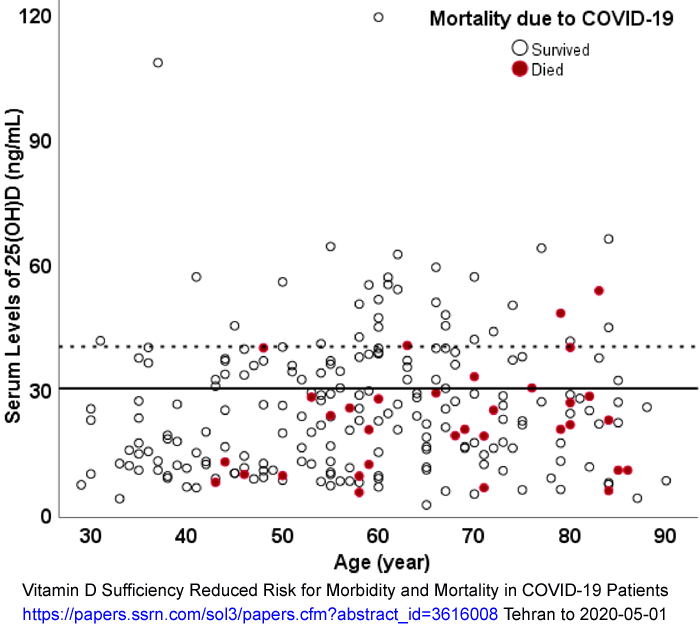
https://aminotheory.com/cv19/ especially the Iranian research linked to and discussed at:
https://aminotheory.com/cv19/#2020-Maghbooli
where 25OHD levels above 30ng/ml are shown to be protective against
COVID-19 severe symptoms, but where some patients with levels of
40ng/ml and higher still die.
Patients with 30ng/ml or more 25OHD had lower severity and death rates than those with less than this.
This what we need to understand. The sharp relationship between
deaths and 25OHD levels depicted in the bogus Prabowo Raharusun Lorenz
Borsche and Dr Bernd Glauner graph above gives a completely false
picture of the relationship. The bogus graph, if believed, gives
us a
false sense of security
that if we could just get everyone above 32 or 35ng/ml there would be
few, if any, deaths from COVID-19.
I am sure that if we could get everyone in a given country to 30ng/ml
25OHD, that symptoms severity would be greatly improved. Also, I
think the amount of virus shedding would be greatly reduced so the
infection rates would drop, rather than keep growing, as has happened
over summer in the UK and the whole EU, with infection rates now rising
as the Sun heads south again and vitamin D levels drop:
twitter.com/Covid19Crusher/
However, it would be better still if we got everyone to at least
40ng/ml. For some people, there would be little or no difference
in general health, all through their life, between 30ng/ml and
40ng/ml. However, for some - especially those with particular
genetic characteristics, or obesity, or when they are 70+, 40ng/ml will
be better for them than 30ng/ml. Within that set, some
people, will be better with 50ng/ml than 40ng/ml and so on.
For some of those infected, 30ng/ml will help them a lot more
than 20ng/ml, but it is not a get-out-of-trouble-free card, as the
Iranian data shows.
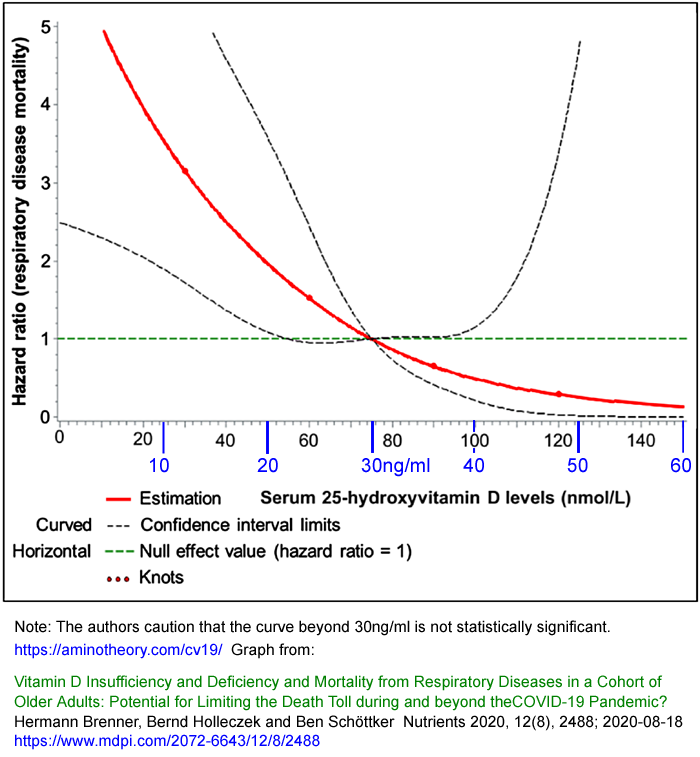
I proposed a long downward-sloping 25OHD vs risk of COVID-19 harm curve (red line in second graph) on 2020-07-28:
https://aminotheory.com/cv19/#hazard
. I was happy to see a similar hazard curve (also in red)
in this article which was published on 2020-08-18. I am yet to
write about this article, which concerns
pre-COVID-19 respiratory tract infections:
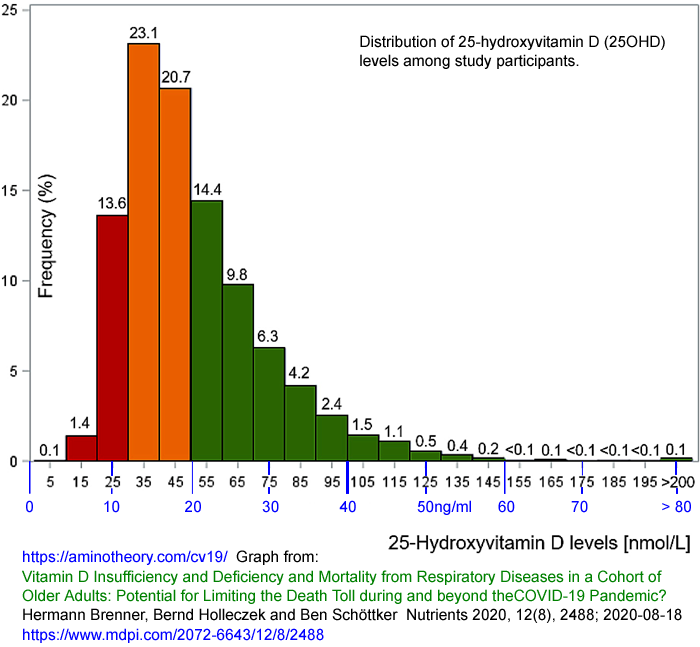
Vitamin
D Insufficiency and Deficiency and Mortality from Respiratory Diseases
in a Cohort of Older Adults: Potential for Limiting the Death Toll
during and beyond the COVID-19 Pandemic?
Hermann Brenner, Bernd Holleczek and Ben Schöttker
Nutrients 2020, 12(8), 2488; 2020-08-18
https://www.mdpi.com/2072-6643/12/8/2488
|
I added the ng/ml figures for the horizontal scale.
Also from the same article:
Now to the 2020-08-01 page with the interview video (linked to from the main page of
https://www.powerofd.org) , which links to a
transcript:
The text of this page has many good elements. Dr Redcross advocates
40 to 60ng/ml
(100 to 150nmol/L) 25OHD levels which accords with the best
research. He ensures all his patients supplement with vitamin D3 adequately and
would much rather do this then prescribe drugs. He is
particularly concerned about low vitamin D levels in people with
pigmented skin. He advocates at least 0.125mg (5000IU) a day D3
supplementation and is disappointed to see mainly 0.025mg and 0.05mg
(1000IU and 2000IU) capsules on sale.
Unfortunately, a central part of this page - and apparently of Dr
Redcross's current understanding - is directly based on the 100% fake
Raharusun
and MA16 articles mentioned above. The above page begins with
three dot points, which together with other similar sentences, repeats
much of the material in these two later paragraphs:
As it pertains to COVID-19, researchers in Indonesia, who looked at data from 780 COVID-19 patients, found [1]
those with a vitamin D level between 21 ng/mL (50 nmol/L) and 29 ng/mL
(75 nmol/L) had a 12.55 times higher risk of death than those with a
level above 30 ng/mL. Having a level below 20 ng/mL was associated with a
19.12 times higher risk of death.
Other research [2] [3] suggests your risk of developing a severe case of, and dying from,
COVID-19 virtually disappears once your vitamin D level gets above 30
ng/mL (75 nmol/L). To ignore this seems foolish in the extreme,
especially since vitamin D supplementation is both safe and
inexpensive. |
Ref
[1] is to a
site with a copy of the bogus Raharusun article. Ref
[2] is to Ilie et al.'s country-wide 25OHD COVID-19 mortality
article, which is very broad brush. I don't regard it as concrete evidence for the risk of harm or death
virtually disappearing with 25OHD levels above 30ng/ml - see the Iranian chart above. Ref
[3] is to a 2020-06-22
commentary by Damien Downing which cites, first and second, Mark Alipio's bogus article MA16
above
and the Raharusun article. (I might have done the same on that
date. It was only about then that I started looking at these
articles critically.)
So here we see great work by Dr Redcross being partly corrupted by
quite a high degree of reliance on 100% bogus data.
Furthermore, one of the articles he cites is based on the same fake
data.
The same applies to Dr Mercola, who in the interview says:
But
typically, they're using 30 and shockingly, and a lot of the studies
have been published with this, the results were still
surprisingly and shockingly different for those that had at least 30
nanograms compared to those who were lower, with the respect to the
mortality rate from COVID-19. It was just shocking. It was
like almost a nine to 10 times greater risk of death.
|
This page links to a detailed 46 page report
Stealth Strategies to Stop COVID Cold:
in which (PDF date 2020-08-11) the Raharusun and Alipio fake articles
are also cited. However, these are just two of 185 references.
After updating this web page, I will write to all the PowerOfD website
people pointing them to this critique. I look forward to
updating this account of
academic rot to be in the past tense.
#indon-govt
Important updates 2020-08-13 a:
An Indonesian government document concerning whether a "Dr Prabowo
Raharusun" ever worked at the hospital cited as his affiliation in the
above article
Even if all the authors listed for this
"Raharusun" article were real people, with good publication histories,
we can see from the critiques above that the article cannot be accepted
as a reliable account of real research. Furthermore, the article
was only a preprint, has not been submitted to any journal and the
preprint has been withdrawn.
Therefore, I suggest, the only reason for citing this article anywhere
is to mention that according to all the available evidence it should
not be considered a reliable account of actual research.
This is a polite, minimal statement about an article which is a
deliberate fake.
Following the publication of the three MDs' article I was party to a
number of email exchanges involving one of the three MDs and a number
of people who doubted the veracity of their article: that is, they
still tentatively or absolutely believed in the existence (and recent
death) of "Dr Prabowo Raharusun" and so in the veracity of the
article
Patterns
of COVID-19 Mortality and Vitamin
D: An Indonesian Study.
I thought such positions to be entirely at odds with all the
evidence. I am not sure that they had taken the time to
read this web page. The wider situation is that all three
articles discussed here, and sometimes one or more of the other Mark
Alipio articles concerning vitamin D and COVID-19, were still being
cited in numerous peer-reviewed (or in the process of being reviewed)
articles as if they were legitimate research reports.
This integration of bogus articles into the fabric of proper research
is an appalling development. Some authors continued to cite the
articles even though they had been withdrawn, without any note to this
effect.
In order to try to reduce these corrosive practices, the three
Indonesian MDs went to some further trouble. They contacted the
director of the hospital cited in the "Raharusun" article and obtained
signed statements from her in both Indonesian and English regarding
this supposed "Dr Prabowo Raharusun". Then they made this
document available at an Indonesian government website as evidence of
the veracity of the director's statement.
In what follows, I have assumed that the statement by the hospital
director is entirely true, and that this corroborates the article of
the three doctors, as well as my own inability to find any sign that
this so-called "Dr Prabowo Raharusun" ever existed.
From this, a number of important things can be reliably ascertained:
- The three MDs did contact the hospital before completing their article.
- The hospital has no record of a doctor of this name.
- The hospital has had no involvement with any research project as described in the "Raharusun" article.
- The hospital does not have and never has had a website.
- The website I and other people referred to, assuming it was the hospital's website, was a deliberate fake.
Points 4 and 5 came as a surprise to me. I discuss the fake website and its contact details in the next section.
The document begins with the three MD's article, followed by the RR
initial version of the "Raharusun" article. Pages 21 and 22 are
the Indonesian and the English versions respectively of the statement
by the director of the hospital.
The PDF document's name is:
Pencatutan
RSUD Sukamara di salah satu artikel yang berjudul Patterns of Covid-19
Mortality and Vitamin D _ An Indonesian Study.pdf
(PDF date 2020-08-07, 898,598 bytes.)
The website it is located on is:
http://ppid.sukamarakab.go.id
. However (on 2020-08-13 at least) this server only responds to
http and https requests (and pings) from IP addresses deemed to be in
Indonesia. While Google's search engine spider has accessed
it in the past, as far as I know, it cannot be accessed
directly
from most or all computers outside Indonesia. In order to access
it from outside Indonesia, a proxy server or VPN router in Indonesia is
required. I know one person who used another proxy server in
Indonesia without success. This one suffices:
If you use your browser to access this proxy server site, and then in
the "Enter URL" box there, type or copy and paste the following URL:
http://ppid.sukamarakab.go.id
you will see the home page of this server, a screenshot (2020-08-13) of which is
here, showing a link to the document we are interested in under the heading
Informasi Terbaru (
New Information). The heading of the link is as follows and in Google translation to English:
Pencatutan RSUD Sukamara di salah satu artikel yang berjudul Patterns of Covid-19 Mortality and Vitamin D : An Indonesian Study
RSUD Sukamara
Recording of Sukamara Hospital in an article entitled Patterns of Covid-19 Mortality and Vitamin D: An Indonesian Study
Sukamara Hospital
This link doesn't work (at least for me) in this proxy system, and
neither does the proxy's URL bar, so to reach the document page, reload
the proxy's home page
https://proxy.web.id
and type or copy and paste this URL into the proxy-server's "Enter URL"
bar, and then click the "Go" button or press the "Enter" key on your
keyboard:
http://ppid.sukamarakab.go.id/front/dokumen/detail/500074980
Here is a
screenshot
of what you should see. Now, you should be able to click
the "Download File" button and read and save the PDF. Here is a
screenshot of page 22: the English version of the letter from the
director of the hospital, RSUD Sukamara, to one of the three MDs:
#R-hospital-website
Important updates 2020-08-13 b: The hospital website at which I and other people were looking was fake
During at times acrimonious email
discussions with various people in early July 2020, all those involved,
including me, were looking at a website which disappeared in mid to
late July.
Its URL was: http://rsudsukamarakab.net . Here is how you
can view a screenshot from the homepage or that site, from
2020-07-10. Click the following link, which is not to any
file, and then delete the Z from the end of the file address, and get
your browser to load that, the correct URL. (I have done this to
avoid search engine spiders finding this image.)
The site was running Wordpress and evidently had pages added as early
as 2017. I found a few links to this site, such as from Facebook
pages, in 2017 or 2018, so evidently this site as we saw it in June and
July 2020 had been in existence since 2017, though we can't be sure
exactly what it looked like then. It is not archived in
https://archive.org
, which as far as I know only occurs if the site owner writes to
archive.org, proves they own the site to them and requests it not be
archived.
On 2020-08-14 I could still find Google's search engine caching pages and images from this site:
Search-1.pngZ and
Search-2.pngZ (Again, click the link, delete the 'Z' and hit "Enter".)
The website only appeared because there was a server, with all the
files which made the website AND because whoever controlled the domain
rsudsukamarakab.net configured the DNS (Domain Name Service) zone file
for that domain to point to that web server. On 2020-08-14,
looking up the full WHOIS response, such as via
tools.dnsstuff.com
(enter
rsudsukamarakab.net
into the WHOIS/IPSHOIS Lookup box and click the arrow there - then
click the "Detailed WHOIS Response" arrow on the results page) there is
an email address listed as being for the owner of this domain, and it
is not any of the addresses listed below. Screenshot:
zyxwvut.pngZ .
From my 2020-07-10 screenshot of the website which appeared to me and
others as being of the hospital, here are the email and phone details:
(The 26542 and 26752 numbers can also be seen in the Search-1 screenshot above.)
Until 2020-08-13 I assumed this website was of the hospital. Then
I read - as you can see above - that the hospital has no website.
The 26752 number matches that on the hospital letterhead. The (fake) hospital website displayed three email addresses:
admin@rsudsukamarakab.net
rsud.sukamara@yahoo.com
info@rsudsukamarakab.net
none of which match the one email address on the letterhead:
rsud_sukamara@yahoo.com
The dot and the underscore make these two totally different Yahoo email addresses.
During email discussions about the veracity of the "Raharusun" article
one person and later a second reported that they had written to the
hospital email address inquiring about the late "Dr Raharusun" who they
had been told (by emails from his colleagues and others who knew him,
including Mark Alipio) had died. The replies they received were
officious but sad confirmation that he had worked at the hospital and
that he had died. One of these replies was forwarded to me.
So I wrote to the admin address about this and received a similar
reply. I didn't believe it and hypothesised that the hospital had
somehow lost control of its domain and that whoever then controlled it
were part of, or were cooperating with, whichever one or more
individuals was encouraging some people to sincerely believe that "Dr
Prabowo Raharusun" person really had existed, and had since died.
I didn't pursue this any further, since my aim was to explain to people
my reasons for considering all these articles fake - and my analysis of
the text of the articles provided more than sufficient evidence to
establish this.
On 2020-08-13 and subsequently, because of the PDF mentioned in the
previous section, I believe that the domain and its website, and so the
three email addresses above, were all the work of some persons who were
not employed by the hospital. The site certainly looked to me
like an official hospital site (given this was a small hospital in a
remote rural part of a developing country). The reply I received
was evidently written to give the impression that it was sent by an
authorised member of the hospital staff.
I have no idea why anyone would create a fake site like this - and
apparently do so for three years or more. It cannot be a
friendly gesture, since the email addresses do not match that of the
hospital. Nor do I understand why a hospital would not have a
website or take action to shut down an unauthorised site such as
this. However, I have no experience of places such as rural
Kalimantan.
Dr Pranata also directed my attention to this Indonesian Ministry of Health listing for the hospital:
This has the same email address and phone/fax numbers as on the hospital letterhead.
This is one of 9 hospitals in the area listed at:
some others of which list no email address or website.
#G-critique
An article by a second
group of authors with no publication history - from India
There is another article on the SSRN preprint server which I had
previously looked at only briefly. I decided to evaluate its veracity in late June 2020.
I took this
snapshot
of the page (2020-06-30), in case it disappeared. The background
image states UNDER REVIEW BY SSRN. The PDF has the full, four MD,
author list:
Vitamin
D Level of Mild and Severe Elderly Cases of COVID-19: A Preliminary
Report
El James Glicio, MD; Siddharth Neelam, MD; Rajeev Rashi,
MD; Deepak Ramya, MD
No date on the PDF, but 2020-05-05 on the SSRN page. (Not peer-reviewed.)
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3593258
PDF creation date is 2020-05-05 19:28.
|
Update 2020-07-06: This article was withdrawn in early July. I wrote to SSRN enquiring as to why, and will report any answer I get here.
This article follows the pattern established by many of the Mark Alipio articles and by the Indonesian article.
A vaguely defined source of clinical
data - the two hospitals are not named, but are in "South
Asia". 176 patients had vitamin D levels recorded pre-hospital, from an initial set
of 672. (This seems highly unlikely to me.) There are no details on
the selection criteria of the initial 672, or what sorts of wards they
were in. There is no information on the range of dates in which data was
collected.
General discussion with references, including the Mark Alipio article
16 and the Indonesian article. Analysis of the data . .
. There seems to be rather sharp upper and lower cutoffs in
the scatter plot of BMI in Figure 9 - so this does not look like real data to me.
I can find no reason to believe this article represents real research.
#disappeared
Disappearing articles
On 2020-08-13 I went through some links
above to find out what had disappeared on various websites since the
page was established on 2020-07-01. All these items concern Mark
Alipio:
- Google Scholar citations URL.
- Twitter profile.
- PDFs of articles 01, 02 and 03 at Academia.edu.
- PDFs of articles 14, 18 and 21 at SSRN.
2020-08-20: Mark Alipio's most cited fake article number 16
disappeared from the SSRN site a day or two ago, as has his profile
page.
Update history
2020-07-01 Initial version. I updated this several times.
2020-07-13 Revised,
simplified version focusing on the text and diagrams of the articles,
but also looking at the publication history of Mark Alipio, the content
of his articles, and on what I later found out about the Indonesian
hospital, and how different this was from what I had initially assumed,
with little or no thought.
2020-07-28 Linked to the British Journal of Nutrition article.
2020-08-03 Added three points from Dr Pranata at:
#R-critique .
2020-08-10 Added notes
#MA13-similar about how to determine whether a journal is predatory or a legitimate open-access journal, with regard to the
International Journal of Engineering Technology Research & Management predatory journal in an article similar to Mark Alipio's 13th article appears.
2020-08-13 Added two new sections concerning the "Raharusun" article:
#indon-govt and
#R-hospital-website . A new section directly above lists items which this page's links point to, but where the item no longer appears.
2020-08-16 Added
publication histories for the three Indonesian MDs. Noted that
the fundraiser had finished, but that the page still exists.
There has been a flurry of email correspondence in the last few days,
including with the Davao Doctor's College, who attest that Mark Alipio
was not associated with them after November 2019. "Our school is
not party to nor does it support any of the supposed undertakings of
Mr. Alipio."
2020-08-20 Mark Alipio's
best known article MA16 has disappeared from the SSRN preprint server
as has his profile page. His image is no longer on rotation
in the "Topnotcher's Corner" of the Davao Doctors' College homepage.
Lorenz Borsche contemplates that this whole affair may have been a scam, and updates the fundraiser page:
#fundraiser-2020-08-20 .
I added the
#academic-rot section which primarily discusses the new and promising
https://www.powerofd.org site's mistaken reliance on the fake Raharusun and Alipio articles and the Raharusun-Borsche graph.
To the home page of this site: ../
©
2020 Robin Whittle Daylesford, Victoria,
Australia
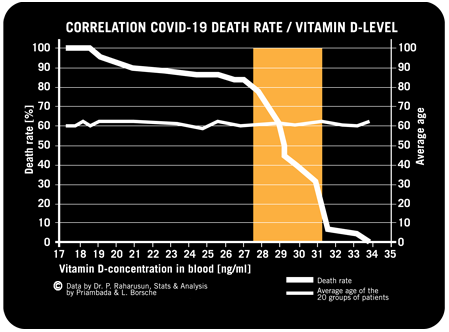
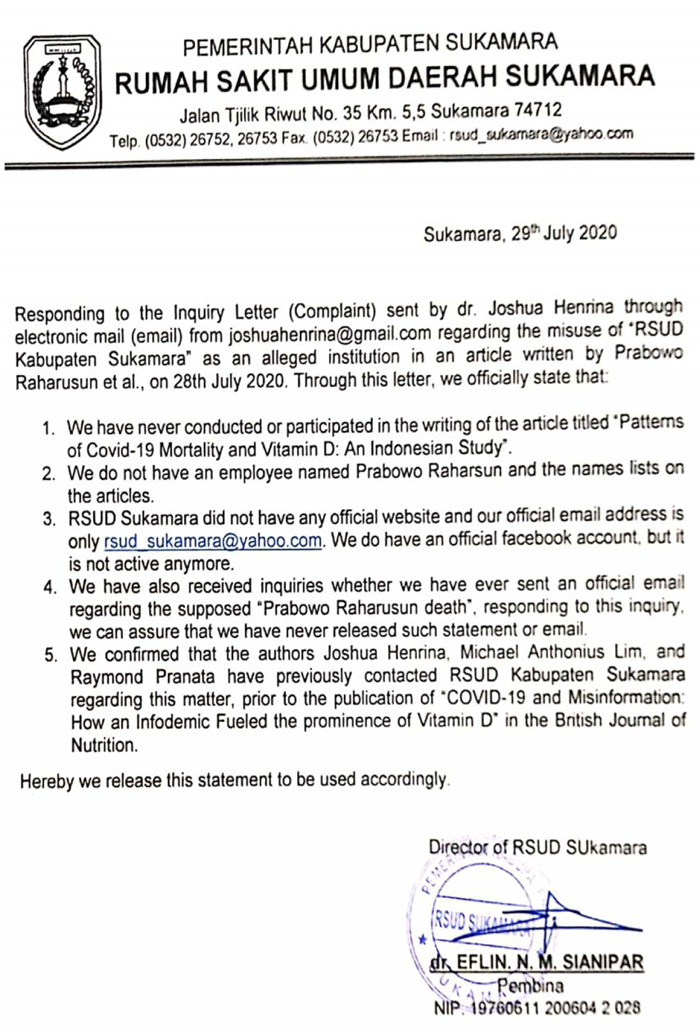
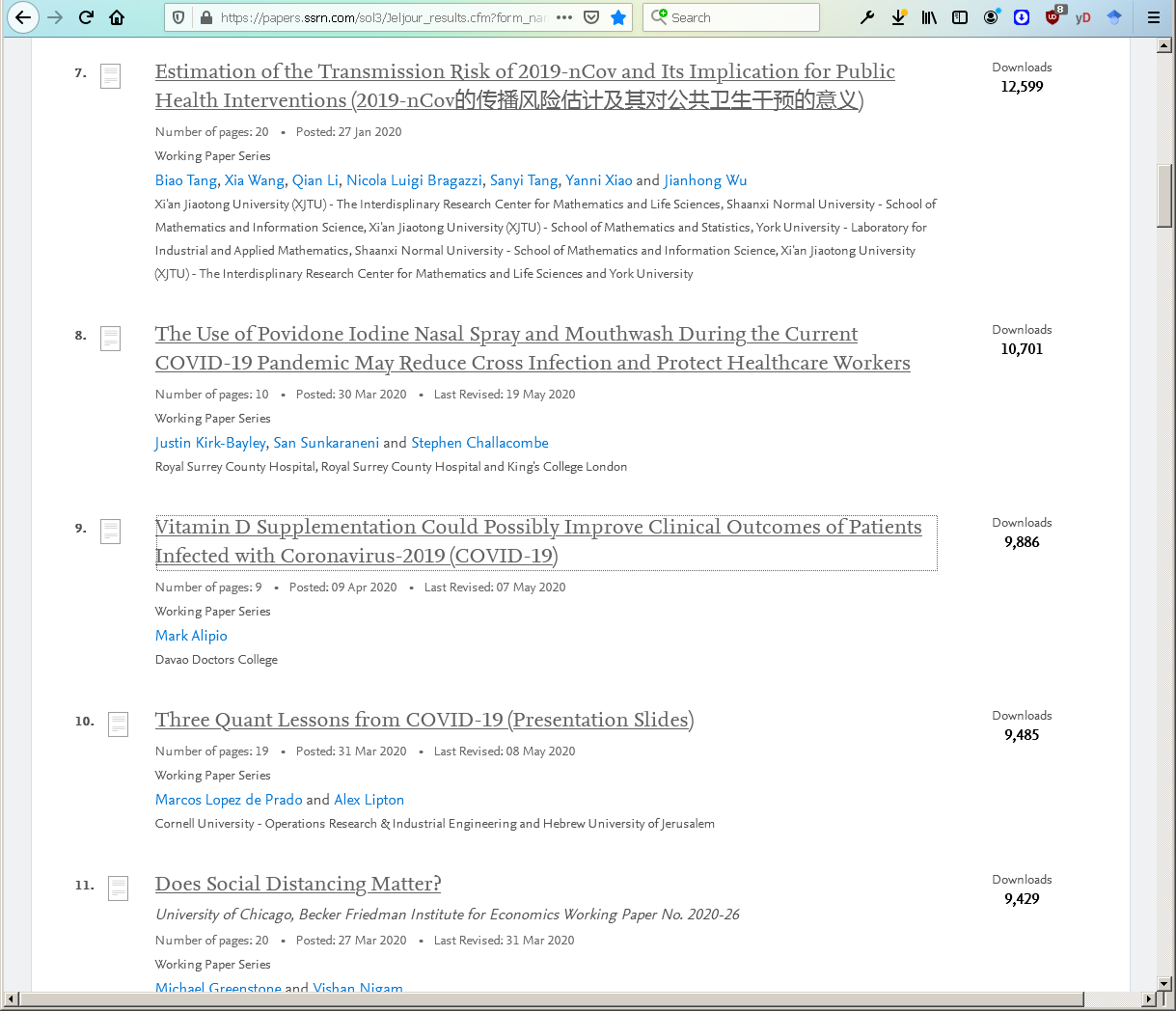{kind=link}
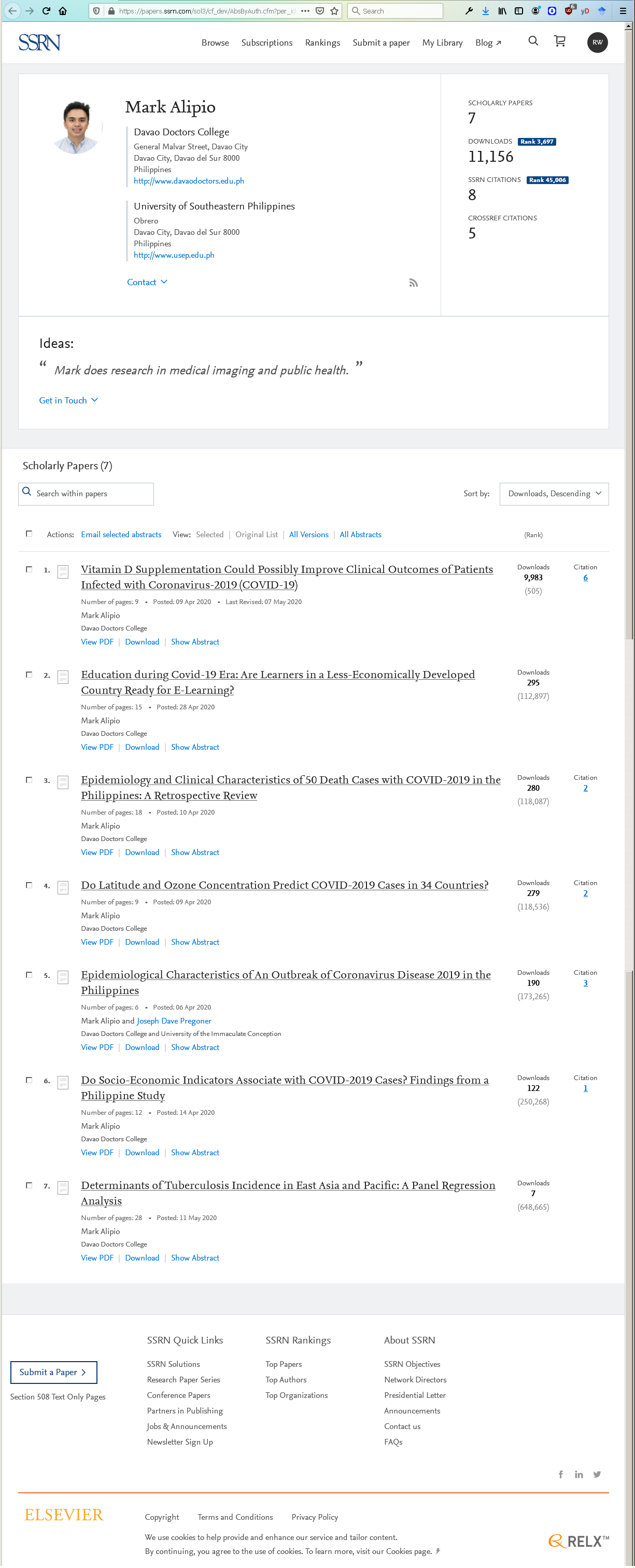{kind=link}
{kind=link}
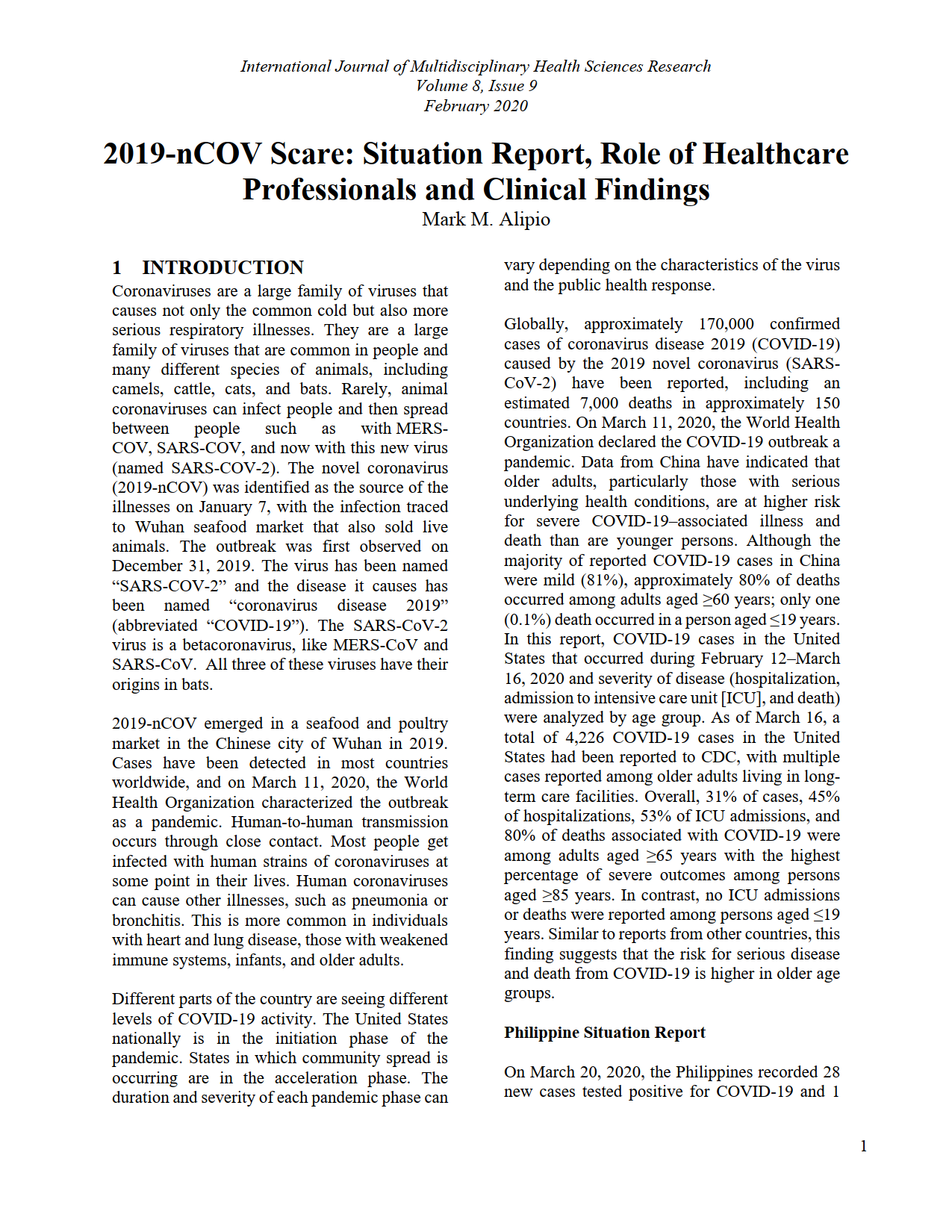{kind=link}
{kind=link}
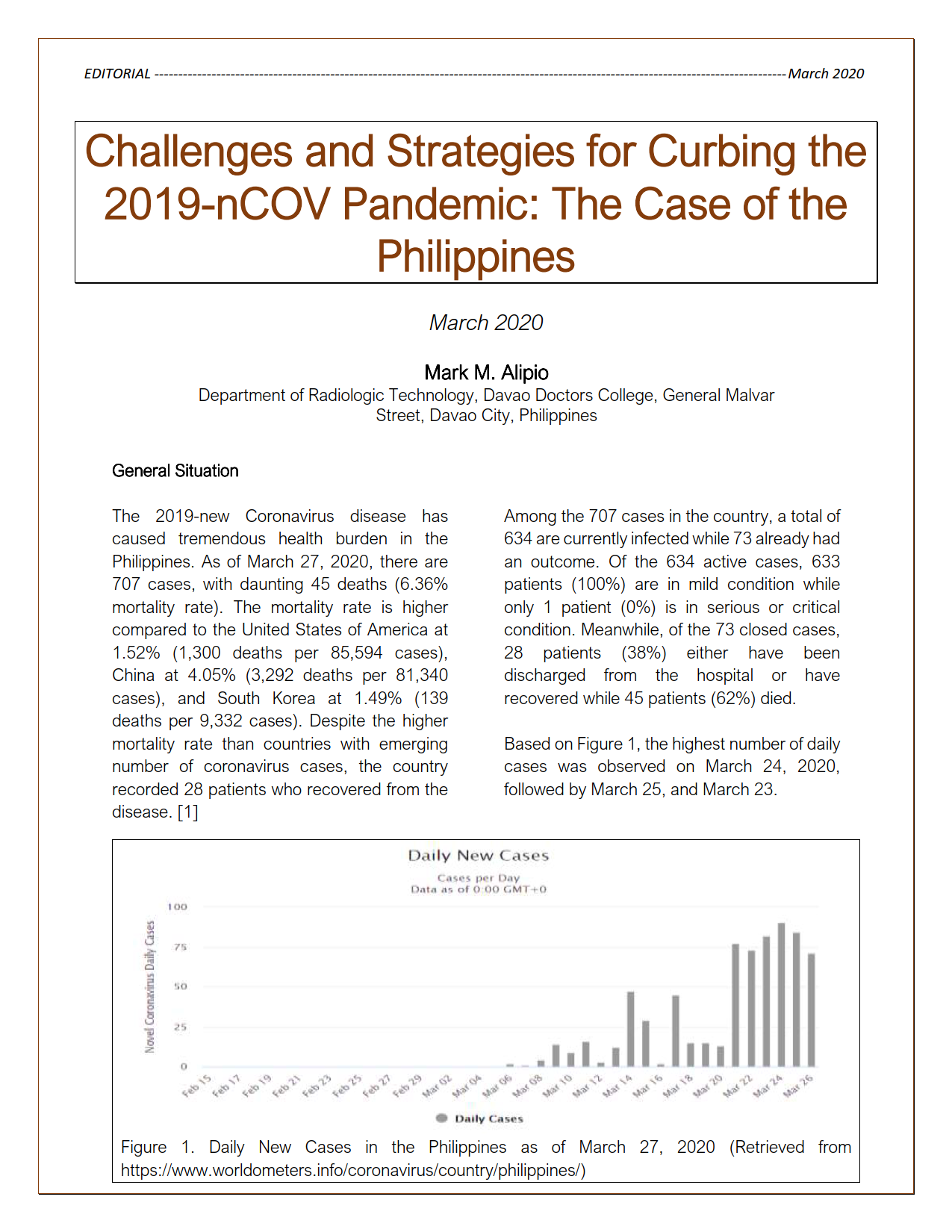{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}